The SI joint has, after much debate, regained the status of a true diarthodial (synovial) joint capable of some movement. The joint is composed of an auricular-shaped surface with an upper vertical and lower horizontal section. A synovial membrane covers the lower two thirds (ventral portion); the upper third (posterior) is mainly fibrous without synovial tissue. Stability is largely ligamentous.
Movement:
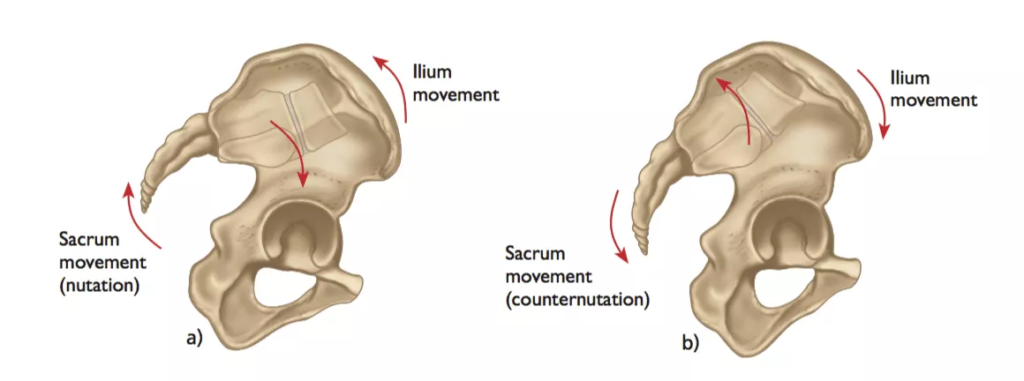
Nutation and counter nutation
Nutation involves an anterior posterior movement around the transverse axis. Thus, when rising from a recumbent position, the sacral promontory moves forward a few milimeters. This also occurs unilaterally, so that when standing on one foot, the SI joint on the side of the weight bearing reaches maximum nutation.
The most common symptoms include:
- Pain is usually localized over the buttock
- Patients can often complain of sharp, stabbing, and/or shooting pain which extends down the posterior thigh usually not past the knee.
- Pain can frequently mimic and be misdiagnosed as radicular pain
- Difficulty sitting in one place for too long due to pain
- Local tenderness of the posterior aspect of the sacroiliac joint (near the PSIS)
- Pain occurs when the joint is mechanically stressed eg forward bending
- Absence of neurological deficit/nerve root tension signs
- Aberrant sacroiliac movement pattern
- Patients will frequently complain of pain while sitting down, lying on the ipsilateral side of pain, or climbing stairs
*** The medical information on this site is provided as an information resource only, and is not to be used or relied on for any diagnostic or treatment purposes. ***